
Our Caring Temple, MD Pediatric Podiatrist Specializes in Children's Foot & Ankle Conditions
PEDIATRIC / ADOLESCENT FOOT CARE
CHILDREN'S FEET SHOULD NOT HURT.
If your son or daughter is not participating as often in sports or in other physical activities or is complaining of foot pain, don't think it's caused by "growing pains". Your son or daughter may have a common developmental foot condition such as flat feet that could be simply treated with a custom foot orthotic.
In addition, parents may observe that their children are often falling or tripping and not able to keep up with normal activities. This may be due to a condition called in-toeing or out-toeing. Many childhood foot conditions can be helped with custom foot orthotic which is an insert that fits into the shoe that keeps the bones in the feet in their proper alignment. This can eliminate their foot pain and allow normal development as your child matures into adulthood.
We treat a wide variety of childhood foot & ankle conditions including:
IN-TOEING & OUT-TOEING
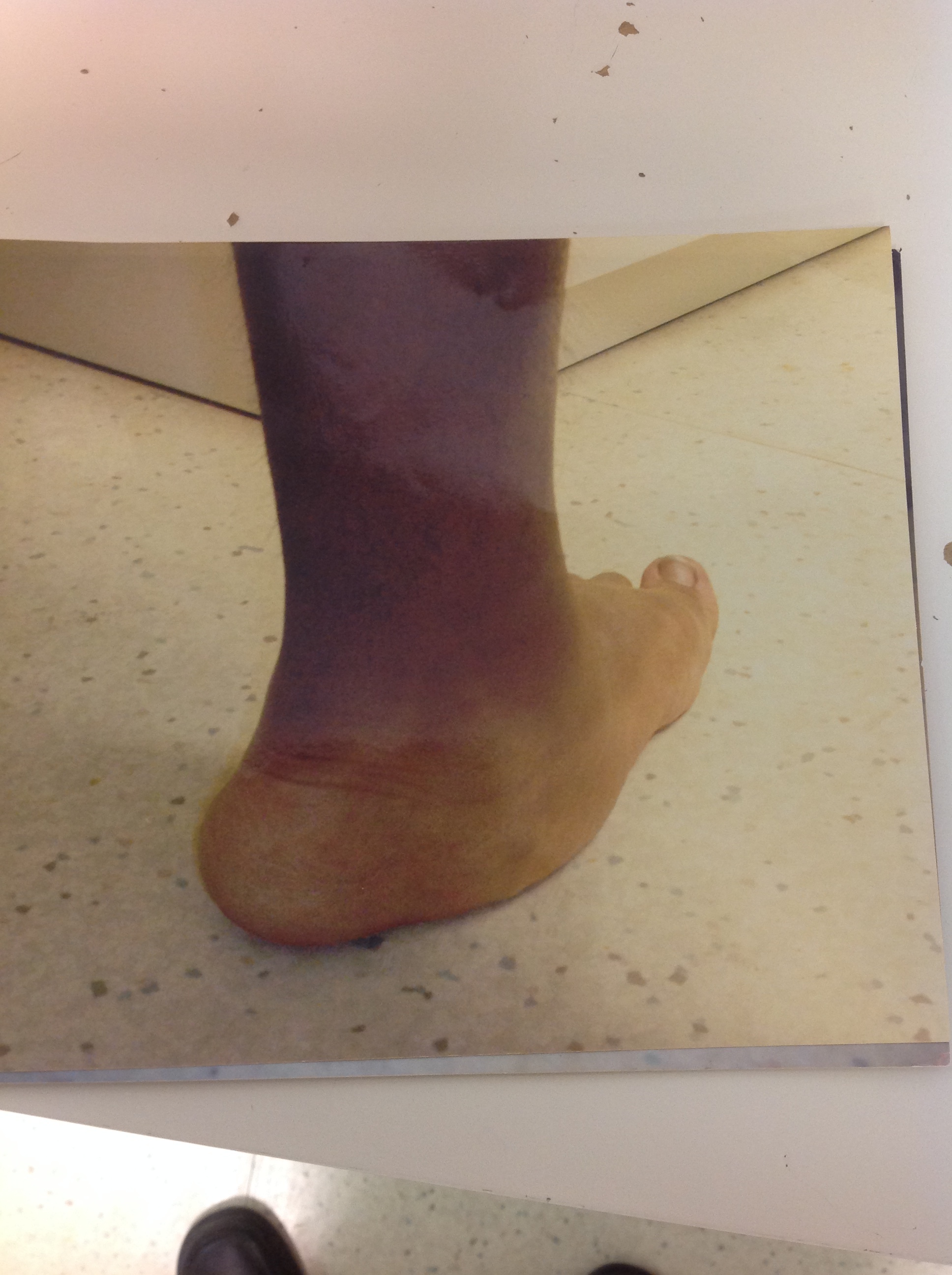
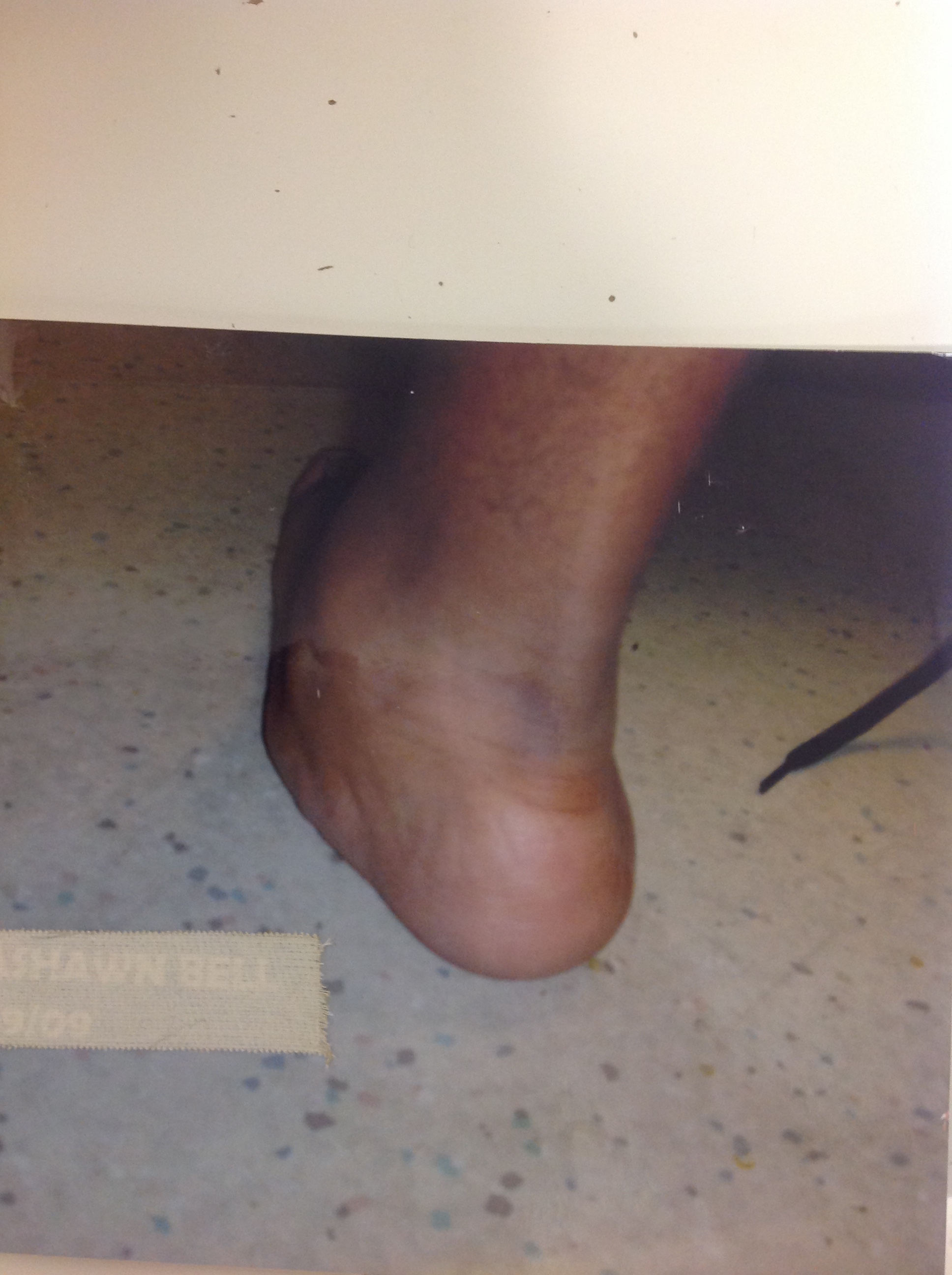
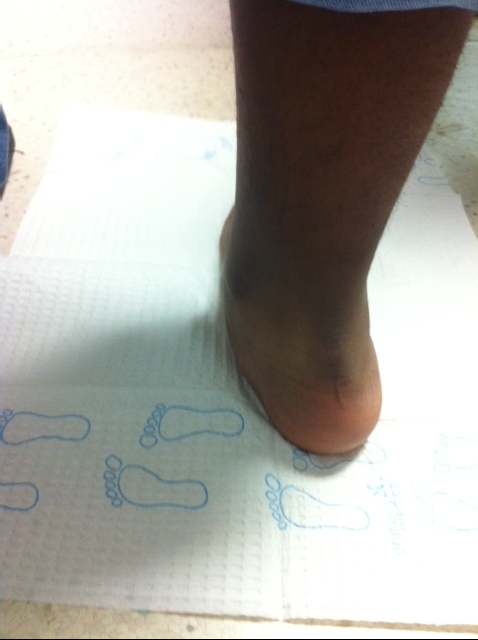
SEVER'S DISEASE
SEVER’S DISEASE AND ACHILLES TENDON
if children seem to have foot pain, problems ambulating, an unusual gait and feet that look to be in poor health, its best to contact a podiatrist
So, if your child is complaining of foot pain, problems ambulating, an unusual gait and feet that look to be in poor health, its best to schedule an appointment with Dr. Burton J. Katzen, DPM, LLC for an evaluation and help them enjoy healthy happy feet in the years ahead.
FLAT FEET
Flat feet are a common condition in infants and toddlers. Most feet are flexible and an arch appears when children begin standing on their toes. The arch continues to develop throughout childhood, and by adulthood most people have developed normal arches. Flat feet are generally associated with pronation, a leaning inward of the ankle bones toward the center line. Shoes of children who pronate, when placed side by side, will lean toward each other after they have been worn long enough for the foot position to remodel their shape.
Flat feet, fallen arches, or “pes planus” is normally a symptomless and fortunately painless condition. When pain in the foot, ankle, or lower leg does occur, especially in children, the feet should be evaluated. Painful progressive flatfoot, otherwise known as tibialis posterior tendonitis or adult-acquired flatfoot, refers to inflammation of the posterior tibial tendon. This condition arises when the tendon becomes inflamed, stretched, or torn. Left untreated, it may lead to severe disability and chronic pain. People are predisposed to tibialis posterior tendonitis if they have flat feet or an abnormal attachment of the tendon to the bones in the midfoot.
Non-steroidal anti-inflammatory medications, icing, physical therapy, supportive taping, bracing, and orthotics are common treatments for painful progressive flatfoot.. In some cases, surgery may be needed to repair a torn or damaged tendon and restore normal function.
If you are suffering with flat feet pain please make an appointment for a comprehensive evaluation.
PERMANENT CURE FOR FLAT FOOT
Exciting Out-Patient Permanent Cure
Hyperpronation is a very common condition of excessive motion of the rear foot which causes the appearance of a “collapsed arch” upon weight bearing. This motion leads to deformity of the foot and potentially knee, hip, and back problems. It occurs with every step a person takes and eventually leads to damage to the musculoskeletal system. This is why most people develop lower extremity symptoms by middle age, or even earlier depending on the degree of deformity. In other words, if your feet are “out of alignment”, sooner or later the effects will be felt.
Hyperpronation is present at the time of birth, and the age of onset of the symptoms depends on the degree of deformity. A child with a flatfoot may develop so called “growing pains” which is caused by abnormal excessive activity of the leg muscles required to propel the foot during normal ambulation.
TREATMENT OPTIONS:
You should not wait to have pain or deformities to treat hyperpronation. As with any other deformity, the sooner treatment is initiated the better the outcome. Oral medications do not address the underlying deformity which is excessive motion of the ankle bone (talus) on the heel bone (calcaneus). Historically, arch supports have been the “gold standard” in treating abnormal foot motion. This type of treatment has been very successful in preventing the abnormal motion, but do not address the underlying internal cause of the deformity to afford a permanent cure. The other disadvantage of arch supports is that they will limit the shoes you may wear (no sandals or high heels) and when you are not wearing the supports, you will not be getting any correction of the deformity or relief of symptoms (ex. Barefoot).
SUBTALAR ARTHROERESIS:
THE IMPLANT RE-ESTABLISHES THE SINUS TARSI SPACE FOUND IN A NORMAL FOOT.



Subtalar arthroeresis is a very viable in office treatment option for the permanent correction of hyperpronation for anyone over the age of three years. The procedure involves placing a small medical grade titanium implant in the sinus tarsi, which is the opening between the talus and calcaneus. This acts as an “internal orthotic” to prevent the abnormal motion (collapse) between the two bones. The titanium is tolerated by the body without ill-effects. It is specifically designed to fit securely into the sinus tarsi without any type of internal fixation (ex. screws, pins, etc.). It does not deteriorate over time or set of a metal detector. It is stronger than bone. The procedure takes approximately 10-15 minutes and is performed though a small ¾ inch incision on the outside of the foot in an office or outpatient ambulatory center. It may be performed under local anesthesia or local anesthesia with light IV sedation. Also, since no boney structures are being disturbed, the procedure is totally reversible.


Post operatively, little pain medication is usually required. Partial weight bearing is allowed the day after surgery, and patients may return to shoes as tolerated after the first redressing usually 4 or 5 days after surgery. Sports activities can be increased to tolerance four weeks after surgery. Usually, orthotics are no longer necessary following the procedure. Contact us today for more information.